


Abstract
Systemic vasculitides comprise a group of autoimmune diseases affecting blood vessels, including large vessel vasculitis (LVV) and medium-sized vessel vasculitis such as giant cell arteritis (GCA) and Takayasu arteritis (TAK). GCA frequently overlaps with polymyalgia rheumatica (PMR), a rheumatic inflammatory condition affecting bursae, tendons or tendon sheaths, and joints. 18F-FDG PET/CT plays an important role in the diagnostic work-up of GCA, PMR, and TAK and is increasingly used to monitor treatment response. This continuing education article provides up-to-date guidance on the role of 18F-FDG PET/CT in patients with LVV, medium-sized vessel vasculitis, and PMR. It provides a general introduction on the clinical presentation and challenges in the diagnostic work-up of LVV and medium-sized vessel vasculitis, with a focus on the 2 major LVV subtypes: GCA, including PMR, and TAK. Next, practice points to perform and interpret the results of 18F-FDG PET/CT are described in line with the published procedure recommendations. Furthermore, the diagnostic performance and its role for treatment monitoring are discussed, taking into account recent international recommendations for the use of imaging in LVV and medium-sized vessel vasculitis in clinical practice. This is illustrated by several clinically representative PET/CT scan examples. Lastly, knowledge of limitations and pitfalls is essential to understand the role of 18F-FDG PET/CT in LVV, medium-sized vessel vasculitis, and PMR. Challenges and opportunities, as well as future research and conclusions, are highlighted. Learning objectives provide up-to-date guidance for the role of 18F-FDG PET/CT in patients with suspected LVV, medium-sized vessel vasculitis, and PMR.
The autoimmune vasculitides encompass a heterogeneous group of diseases characterized by inflammation of blood vessels. Classification is based on the size and the type of vessels that are preferentially affected by the specific type of vasculitis (1). The main forms of large vessel vasculitis (LVV) include giant cell arteritis (GCA) and Takayasu arteritis (TAK). GCA is the most common form of vasculitis in European populations, with the highest lifetime risk (i.e., 0.5%–1%) among people of Northern European descent (Figs. 1 and 2) (2). In contrast, TAK is more common in Asian populations (Fig. 3) (3). GCA and TAK more often affect women. One important distinction between GCA and TAK is the age of disease onset. TAK primarily occurs before the age of 40, whereas GCA affects individuals after the age of 50, with a mean age between 70–75 y (Fig. 4). Furthermore, GCA frequently overlaps with polymyalgia rheumatica (PMR), a rheumatic inflammatory condition affecting bursae, tendons or tendon sheaths, and joints (Fig. 5) (4–6). PMR may also occur in the absence of GCA and is the most common rheumatic inflammatory condition in the elderly, with an age distribution similar to that of GCA (2).

Digital 18F-FDG PET/CT of 64-y-old female with suspected GCA. Patient presented with fatigue and claudication of arms. Measurements of systolic blood pressure in brachial arteries varied significantly. Measurements lower than 100 mm Hg and higher than 120 mm Hg were sequentially registered. Duplex ultrasonography showed bilateral stenosis of subclavian and axillary arteries. Patient also complained of morning stiffness and pain in neck, shoulders, and hips. (Left) Maximum-intensity-projection 18F-FDG PET image showing significantly increased uptake (higher than liver) in aorta, carotid, subclavian, and axillary arteries. Increased uptake (similar to liver) may also be seen in femoral and popliteal arteries, as well as around hips and shoulders. (Right bottom) Axial fused 18F-FDG PET/CT images showing significantly increased uptake in suprarenal abdominal aorta. Diffuse and circular uptake is highly suggestive of LVV.

Digital 18F-FDG PET/CT of 80-y-old male with suspected GCA. Patient’s main symptom consisted of both-sided temporal headache, which was accompanied by fatigue. Laboratory investigation showed C-reactive protein of 120 mg/L. (Left) Maximum-intensity-projection 18F-FDG PET image showing strongly elevated uptake (significantly higher than background) in cranial arteries, most notably in superficial temporal and carotid arteries. Elevated uptake (similar to liver uptake) can be seen in subclavian, axillary, femoral, and popliteal arteries. These findings are highly suggestive of C-GCA and LV-GCA. In addition, moderate uptake can be seen around shoulders and hips, suspected for PMR activity. (Right) Axial 18F-FDG PET/CT fusion images of head. (Right top) Elevated uptake in frontal and parietal branches of superficial temporal artery, left posterior auricular artery, and occipital arteries. (Right bottom) Significantly increased uptake in internal carotid and vertebral arteries. Elevated uptake can also be seen at junction of external carotid artery and common superficial temporal artery, as well as maxillary arteries and right posterior deep temporal artery.

18F-FDG PET/CT of 16-y-old female with suspected TAK. Patient had been experiencing generalized malaise. Laboratory investigations showed C-reactive protein of 98 mg/L and ESR of 119 mm/h. Maximum-intensity-projection 18F-FDG PET image shows elevated uptake in thoracic aorta and part of abdominal aorta. ESR = erythrocyte sedimentation rate.

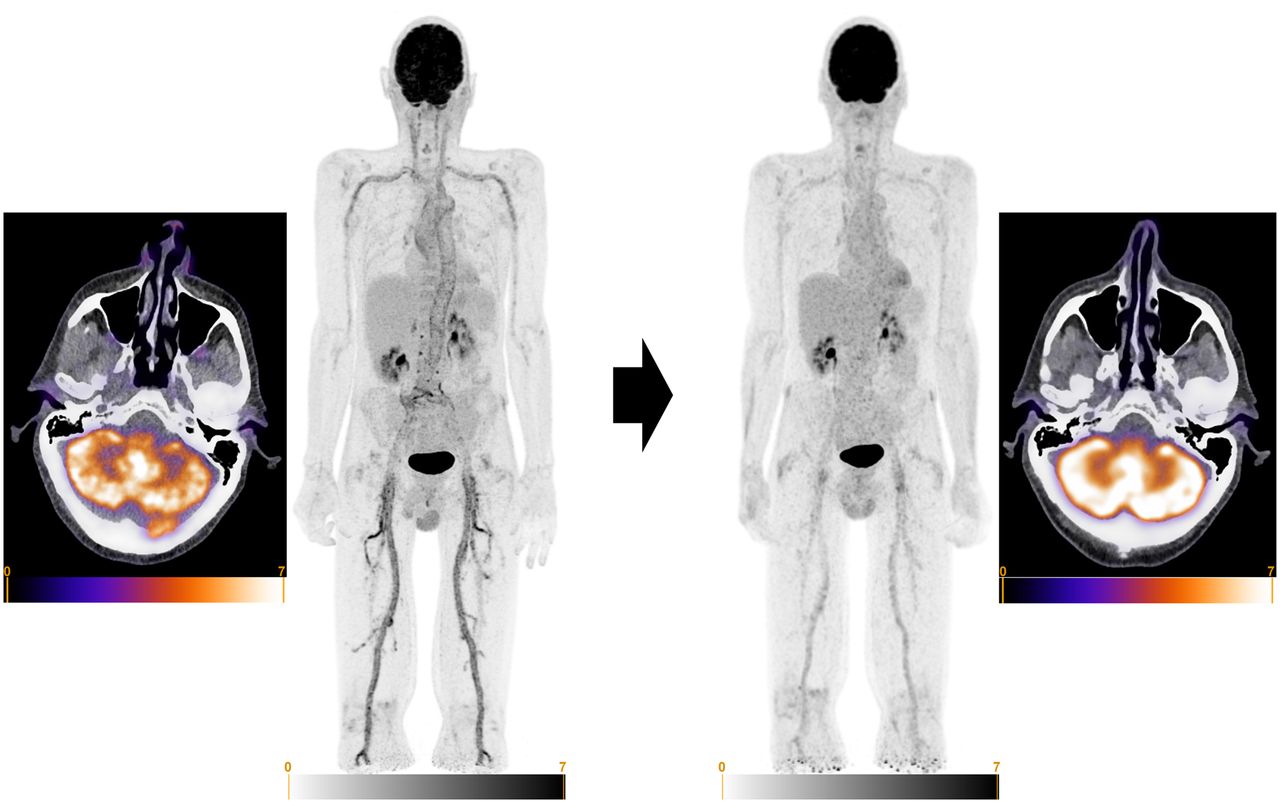
18F-FDG PET/CT imaging at time of diagnosis (before treatment) and after 1 y of treatment in 67-y-old male GCA patient. At time of diagnosis, patient presented with complaints of PMR, accompanied by C-reactive protein (CRP) of 121 mg/L and ESR of 106 mm/h. Patient had been treated with prednisolone and subsequently with methotrexate. At 1 y, CRP remained elevated despite methotrexate treatment. Patient did not experience GCA-related symptoms at that time but had some symptoms of PMR. (Left) Axial 18F-FDG PET/CT fusion image of head and whole-body maximum-intensity-projection (MIP) image at time of diagnosis. Moderately increased uptake (higher than background) can be seen in maxillary arteries. Significantly increased uptake (higher than liver) can also be found in aorta and carotid, subclavian, axillary, iliac, and femoral arteries (PETVAS = 27). In addition, moderately increased uptake (similar to liver) can be observed surrounding shoulders and hips. (Right) Whole-body MIP image and axial 18F-FDG PET/CT fusion of head after 1 y of treatment. Slightly increased uptake (similar to liver) can be observed in aorta and carotid, subclavian, axillary, iliac, and femoral arteries (PETVAS = 13). No uptake was found in maxillary arteries. Moderately increased uptake was found surrounding hip joints. ESR = erythrocyte sedimentation rate.

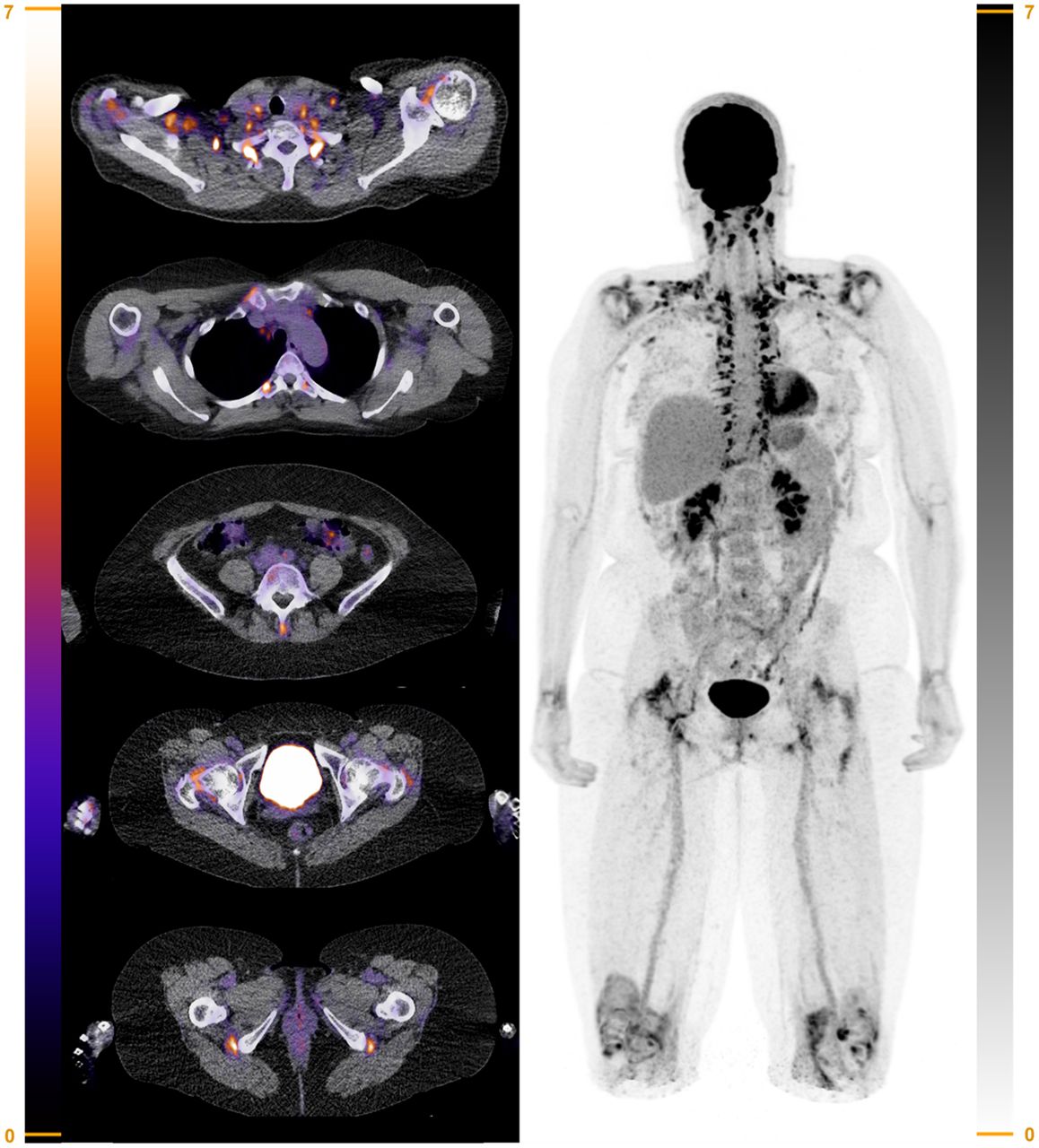
Digital 18F-FDG PET/CT in 59-y-old female patient suspected of having PMR. Patient presented at rheumatology outpatient clinic with pain in neck, shoulders, and hips. She also experienced morning stiffness of 2 h, and her blood inflammatory markers were increased (C-reactive protein, 63 mg/L; ESR, 72 mm/h). (Left) Axial 18F-FDG PET/CT fusion images showing significantly increased uptake (higher than liver) in shoulders, right sternoclavicular joint, lumbar interspinal bursa, hips, and ischial tuberosities. (Right) Whole-body maximum-intensity-projection image showing significantly increased 18F-FDG uptake in shoulders, sternoclavicular joints, lumbar interspinal bursa, hips, ischial tuberosities, and knees. Slightly elevated 18F-FDG uptake may be seen in wrists. Increased 18F-FDG uptake due to brown fat activation can also be seen in neck and paravertebral at thoracic spine (Leuven score = 23, Groningen/Leuven score = 14) (Supplemental Table 1). ESR = erythrocyte sedimentation rate.
Historically, involvement of cranial arteries was thought to be a hallmark of GCA. This is reflected in one of the earlier names of the disease, temporal arteritis, and the American College of Rheumatology 1990 criteria for the classification of GCA, which focused on cranial symptoms and signs and biopsy proof of temporal artery inflammation. This cranial GCA (C-GCA) may give rise to classic symptoms such as headache, jaw claudication, and ischemic visual loss (7), the latter reflecting infarction of the optic nerve related to inflammation of the posterior ciliary arteries (8). With the emerging role of imaging, it has been recognized that many patients with GCA may also have inflammation of the aorta and its major branches and that this large vessel involvement can occur in the absence of cranial artery involvement (9). Consequently, clinicians now classify C-GCA and large vessel GCA (LV-GCA) according to symptoms or affected arteries on imaging (10).
In general, TAK can affect the same vasculature as LV-GCA, although some differences exist. For instance, carotid, mesenteric, and renal artery involvement is more common in TAK. In contrast, temporal artery involvement is less common in TAK, and involvement of the ocular arterial system is rare (11). Patients with LV-GCA or TAK may present with fever of unknown origin, but more specific symptoms such as arm claudication and carotidynia can occur (7,11). Aortitis is an all-encompassing term ascribed to inflammation solely of the aorta (Fig. 6). It includes “true” aortitis limited to the vascular wall and periaortitis and involving the adventitial layer and potentially surrounding fat and other soft tissues. Periaortitis may also present as an inflammatory aneurysm or retroperitoneal fibrosis.

18F-FDG PET/CT of 52-y-old man with history of idiopathic inflammatory abdominal aortic aneurysm for which he underwent prosthetic vascular graft surgery. Patient presented 1 y after surgery with increased C-reactive protein (231 mg/L) and decreased kidney function based on postrenal obstruction. Patient was diagnosed with recurrence of inflammatory aneurysm and received therapy with high-dose GCs and azathioprine. Ureteric obstruction was treated with temporary nephrostomy catheters. Immunosuppressive therapy was tapered in following 2 y. No clinical or biochemical signs of active (peri-)aortitis recurred. (Left) Sagittal and axial 18F-FDG PET/CT fusion images and whole-body maximum-intensity-projection (MIP) image of patient at time of diagnosis (before starting immunosuppressive treatment). Markedly increased, diffuse, and circular 18F-FDG uptake is seen in dilated aortic wall. There is no evidence of inflammatory activity in other locations, including prosthetic graft itself. Right: whole-body MIP image and sagittal and axial 18F-FDG PET/CT fusion images of patient 2 y later after withdrawal of GC therapy. 18F-FDG uptake was significantly decreased compared with time of diagnosis but had not completely normalized.
In all vasculitides, laboratory testing usually shows raised inflammatory markers in the blood. C-GCA can be further demonstrated by temporal artery biopsy, color Doppler ultrasonography (CDUS) of the superficial vessels, and MR angiography (MRA), with recent clinical guidelines suggesting a prominent role of CDUS as a first-line test in suspected C-GCA (12). MRA, CT angiography (CTA), and CDUS can be used for detection of vascular inflammation in LV-GCA and TAK (12). Ultrasonography and MRI of the shoulder and hip girdle may demonstrate inflammation of bursae, tendons or tendon sheaths, and joints in patients with PMR (13–15). In addition, 18F-FDG PET/CT is considered an important tool to demonstrate inflammation in GCA, PMR, and TAK.
Glucocorticoid (GC) treatment is the cornerstone in GCA, PMR, and TAK. High initial GC doses are used in GCA and TAK: typically 40–60 mg of prednisone daily, with 500- to 1,000-mg methylprednisolone pulse therapy on 3 consecutive days reserved for patients with severe ischemic manifestations (e.g., visual loss) (16). In TAK, the clinical guidelines indicate that GC treatment should be combined with other immunosuppressive agents early in the disease. First-line treatment of TAK may consist of conventional synthetic disease-modifying antirheumatic drugs, such as methotrexate and azathioprine (16,17). Anti-TNF and anti–IL-6 receptor therapy may serve as second-line immunosuppressive therapy in refractory and relapsing cases. Treatment guidelines for GCA by the American College of Rheumatology suggest early initiation of anti–IL-6 receptor therapy in all newly diagnosed patients (18), whereas European League Against Rheumatism recommendations advocate the addition of anti–IL-6R therapy in cases of relative contraindications for GC treatment or a relapsing disease course (16). Methotrexate is considered a reasonable alternative for anti–IL-6 receptor therapy, according to American College of Rheumatology guidelines and European League Against Rheumatism recommendations. Patients with PMR are typically started on medium GC doses (15 mg of prednisone) daily (19). GC-sparing immunosuppressants such as methotrexate are usually added when patients with PMR suffer from GC side effects or disease relapse.
ROLE OF 18F-FDG PET/CT ANGIOGRAPHY (PET/CT[A]) IN DIAGNOSING LVV AND PMR
Ultrasonography and MRA are mainly used to detect C-GCA, whereas CTA, MRA, and 18F-FDG PET/CT are useful for detecting LV-GCA in patients presenting with general symptoms (12). However, the new-generation PET/CT scanners, providing superior sensitivity and better spatial resolution, also allows visualization of the cranial arteries by 18F-FDG PET/CT (20,21). 18F-FDG PET/CT can be used in patients with clinical symptoms of C-GCA, LV-GCA, and TAK to visualize which vessels are involved, disease extent and activity, and coexistence of PMR. 18F-FDG PET/CT can also be used in patients without typical clinical symptoms but with persisting fever or inflammation of unknown origin. Vasculitis or PMR can be one of the diseases causing this inflammation or fever.
Normally, low-dose CT is performed in PET imaging for attenuation correction and anatomic localization. However, performing contrast-enhanced CT is also possible according to local practice or guidelines, and newer PET/CT camera systems offer the possibility to perform a CTA directly after the PET acquisition and with the same quality as performed on a single CT camera system. Therefore, PET/CTA combines the unique characteristics of the PET part in visualizing the metabolic activity of the vessel walls and the CTA characteristics of visualizing anatomic changes or stenoses of the vessels in a single imaging modality.
In GCA, a prospective study of 18F-FDG PET imaging in patients with GCA showed vascular 18F-FDG uptake in 83% of patients, particularly at the subclavian arteries (74%) but also in the thoracic and abdominal aorta (>50%) and the femoral arteries (37%) (22). A metaanalysis of 6 studies evaluating 18F-FDG PET for the diagnosis of GCA reported an overall sensitivity of 80% and specificity of 89%. Moreover, the negative predictive value of a 18F-FDG PET scan for GCA was excellent (88%) (23).
18F-FDG PET/CT is also widely used for the diagnosis of TAK (24). One metaanalysis, including patients with TAK, reported a sensitivity of 81% and specificity of 74% for 18F-FDG PET/CT (25). For diagnosing C-GCA, a binary visual 18F-FDG uptake score has been proposed that yields a sensitivity of 73%–83% and specificity of 75%–100% (20,21,26).
18F-FDG PET/CT is an accurate imaging method for distinguishing between aortitis and periaortitis, which is important for identifying the underlying cause (e.g., infectious and noninfectious conditions) (27,28). Mild and heterogeneous metabolic activity of the aortic wall is frequently noticed in the absence of vasculitis, especially in atherosclerotic aneurysms (29). Periaortitis is characterized by a periaortic soft-tissue mass surrounding the aorta and eccentric to the calcifications of the media, visible on radiographic imaging and ultrasound. 18F-FDG uptake is an important indicator of active disease, potentially enabling (treatment) follow-up (30).
18F-FDG PET/CT can also show inflammation of periarticular and articular synovial structures in overlapping PMR or in isolated PMR. Van der Geest et al. (31) demonstrated in a systematic review that 18F-FDG uptake at multiple anatomic sites in the shoulder and hip girdle and spinal column is informative for a diagnosis of PMR.
ROLE OF 18F-FDG PET/CT(A) IN THERAPY MONITORING OF LVV AND PMR
Therapeutic monitoring can be challenging in patients with LVV and PMR, because signs and symptoms and laboratory tests are not specific for these conditions. In addition, inflammatory markers in the blood are often lower during relapse than at diagnosis (32). Imaging tools could thus be of interest for monitoring disease activity during treatment.
Currently, 18F-FDG PET/CT is not routinely recommended for treatment monitoring in GCA and PMR in clinical routine (33). Even though high-dose GC treatment has substantial effects on 18F-FDG uptake after 10 d of treatment (34), it seems that some arterial wall 18F-FDG uptake may persist during treatment-induced remission later in the disease course (35). Nevertheless, most studies show that the extent and intensity of 18F-FDG uptake decrease during treatment. Hence, a metaanalysis suggested that 18F-FDG PET/CT has a moderate sensitivity of 78% and specificity of 71% for distinguishing active from quiescent LV-GCA during treatment (24). A comparable diagnostic accuracy was noted in a recent study with 100 consecutive LV-GCA patients (36). The treatment effect on arterial wall uptake is not restricted to GC treatment, but a similar decrease has been observed in GCA patients treated with methotrexate and anti–IL-6 receptor therapy (37).
Few studies have examined the potential role of 18F-FDG PET/CT for treatment monitoring of PMR, because response to treatment is usually based on a clinical evaluation (38,39). Comparable to arterial wall 18F-FDG uptake in LVV, studies in PMR patients have shown that 18F-FDG uptake at the shoulder and pelvic girdle and interspinous bursae decreases, but not necessarily normalizes, during treatment-induced remission (31).
PET PROCEDURES
Patient Preparation and Scan Acquisition
Optimal patient preparation is crucial (Table 1). Patients must be fasting for at least 6 h and avoid strenuous activity for 24 h before 18F-FDG injection. Blood glucose levels are preferably less than 7 mmol/L. 18F-FDG PET should be performed before GC treatment (unless there is a risk of ischemic complications) or within the first 3 d of treatment. For PET/CT acquisition, low-dose, non–contrast-enhanced CT (for attenuation correction and anatomic reference) is performed from the vertex to the feet (or at least including the knees) 60 min after 18F-FDG injection, with the patient in a supine position with the arms next to the body. It is described that a time interval of 2 h may be even more optimal for PET activity detection in GCA (40). Injected activities, scan duration, or diagnostic contrast-enhanced CT may be performed according to applicable local protocols and guidelines (33).
Patient Preparation and 18F-FDG PET/CT Acquisition
Scan Interpretation and 18F-FDG PET/CT Scores
Several 18F-FDG PET interpretation criteria, both visual and semiquantitative, have been proposed, and there is insufficient evidence that semiquantitative parameters may outperform a visual grading scale to diagnose LVV in routine clinical practice (41). A standardized 4-point visual grading scale (arterial to liver uptake) is recommended with grade 0, no uptake; grade 1, uptake lower than liver; grade 2, uptake similar to liver; and grade 3, uptake higher than liver. Grade 3 is considered positive for LVV, whereas grade 2 may be indicative of LVV (33). In addition, a quantitative composite score, based on the visual grading scale of several individual arterial segments (typically between 7 and 15 segments), could be applied that is known as the total vascular score or PET vascular activity score (PETVAS) (33,42,43). This composite score provides an overall assessment of disease burden, has proven robust with little interobserver variability, and may be preferred for evaluating treatment response. 18F-FDG uptake in cranial arteries are scored as 3-point visual grading (0–2), with grade 0 representing uptake not above the surrounding tissue, grade 1 representing uptake just above the surrounding tissue, and grade 2 representing uptake significantly above the surrounding tissue (21).
In PMR, various 18F-FDG PET scores have been reported. The Leuven score is the best validated one, providing a pooled sensitivity of 89.6% and specificity of 93.3% (Supplemental Table 1) (supplemental materials are available at http://jnm.snmjournals.org) (44–46). The Leuven score is the summed score of visual 18F-FDG uptake at the cervical and lumbar interspinous bursae, sternoclavicular joints, ischial tuberosities, greater trochanters, hips, and shoulders (44). 18F-FDG uptake is graded according to a standardized 3-point visual 18F-FDG grading scale: grade 0, no uptake; grade 1, uptake lower than liver; and grade 2, uptake similar to or higher than liver. A concise version, the Leuven/Groningen score, appears to be at least equally informative for a diagnosis of PMR, only requiring visual assessment of 18F-FDG uptake at the sternoclavicular joints, hips, ischial tuberosities, and lumbar interspinous bursa (45,46). The Leuven and Leuven/Groningen scores also provide excellent interrater agreement (46).
Pitfalls
Blood glucose levels should be as low as possible (preferably <7 mmol/L). Even though hyperglycemia may not have a significant impact on the false-negative rate of 18F-FDG PET for detecting inflammatory lesions (in contrast to oncologic indications), a negative correlation has been observed between blood glucose levels and 18F-FDG arterial wall uptake (47,48).
Oral GC therapy for at least 10 d decreases the sensitivity of 18F-FDG PET for diagnosing LVV, but its sensitivity is not affected when performed within 3 d after oral GC initiation (34). There are no prospective data available on the 3- to 10-d window, and adherence to the 3-d window is recommended to date. In addition, GCs may increase liver uptake, thereby affecting the visual scoring of vascular 18F-FDG uptake (49).
Atherosclerotic vascular uptake, especially in the elderly and at the iliofemoral arteries, may reduce the specificity of 18F-FDG PET for diagnosing LVV (50). Despite the possible overlap between entities, 18F-FDG uptake patterns and the presence of calcifications on CT are helpful to hint toward one or the other: LVV appears as a linear, diffuse, and circumferential uptake, whereas atherosclerosis is characterized by a typical patchy uptake pattern with generally low intensity.
Arterial graft–associated 18F-FDG uptake might raise concerns regarding the diagnosis or disease activity assessment in patients with LVV because the 18F-FDG uptake pattern is similar. However, significant 18F-FDG uptake confined to the arterial graft does not equate to active vasculitis but rather reflects a chronic, low-grade, nonspecific reaction to the graft material (51).
CHALLENGES FOR THE FUTURE AND CONCLUSIONS
Although 18F-FDG PET/CT has become an important diagnostic test in the evaluation of LVV and PMR, various questions regarding its use in LVV and PMR warrant further research. Standardization of 18F-FDG PET/CT scans is crucial, including the complete PET procedure, patient preparation, scan acquisition, scan reconstruction, and image analysis, and standards should be followed and adapted when needed (33). Development of scoring methods for PMR activity on PET is ongoing, and these methods need to be validated in large, prospective cohort studies. Developments in PET/CT camera systems, such as digital or total-body systems, may enhance sensitivity and spatial resolution with a better signal-to-noise (i.e., vessel wall vs. lumen) ratio, including the possibility to scan at later time points while retaining adequate image quality. Furthermore, these new-generation PET/CT scanners allow administration of lower tracer activities to patients while achieving similar or even better image quality than conventional scanners. These systems, including the new-generation PET/MRI scanners, may also visualize pathologic uptake in the smaller cranial vessels (e.g., temporal and vertebral arteries) (20,52). PET/MRI will further reduce the radiation dose, because CT lacks comparable accuracy in GCA diagnosis (53), and it has the advantage of tissue characterization of GCA and PMR, which is of particular value in younger individuals and in (repetitive) monitoring of disease activity (54,55).
Combining total-body systems with more specific immuno-PET tracers for vasculitis would allow more thorough insight into how specific cell subpopulations are involved and behave in the pathogenesis of specific types of vasculitis. Moreover, multiorgan changes regarding kinetic uptake of specific PET tracers after appropriate treatment of vasculitis could be assessed with total-body systems, something that was not possible before the development of this type of scanner (56).
Immuno-PET tracers, binding to specific immune cell subsets, could potentially be more accurate than conventional 18F-FDG for treatment monitoring of patients with LV-GCA (57,58). However, further understanding regarding immune cell subsets in vasculitic lesions is needed for better selection of tracers and targets for tracer development.
Future studies are also needed to investigate the role of 18F-FDG PET/CT in treatment monitoring and as a prognostic factor for LVV and PMR. For instance, studies have suggested that aortic 18F-FDG uptake at diagnosis is associated with an enhanced risk for development of aortic aneurysms many years thereafter (59). Decision-making is always needed in the clinical context. When more specific immuno-PET tracers become available, the question may arise whether therapy should or can be modified based solely on imaging results and whether distinct immunosuppressive treatments have an equal effect on vascular uptake in patients with LVV.
In conclusion, 18F-FDG PET/CT is an important diagnostic tool for detecting inflammation of large- and medium-sized vessels in patients with systemic vasculitides and in PMR. 18F-FDG PET/CT can provide complementary information to other conventional imaging techniques. Furthermore, 18F-FDG PET/CT may have a role in therapeutic monitoring of patients with vasculitis and PMR, but it remains challenging to differentiate remission from smoldering disease activity. A new generation of total-body PET scanners can limit radiation exposure while providing excellent sensitivity. The introduction of immune-cell targeted radiotracers will potentially allow direct visualization of inflammatory cell infiltrates in the vasculature of patients with vasculitis.
Footnotes
Learning Objectives: On successful completion of this activity, participants should be able to (1) understand the role of 18F-FDG PET/CT for diagnosis and therapy monitoring of LVV and PMR; (2) learn about the strengths and limitations of 18F-FDG PET/CT in LVV and PMR, including the pitfalls; (3) know the PET procedures around LVV and PMR; and (4) realize the potential of more specific PET tracers in LVV and PMR, particularly in monitoring disease activity.
Financial Disclosure: Kornelis van der Geest received a speaker fee from Roche and research support from AbbVie. In accordance with ACCME Revised Standards for Commercial Support and SNMMI Conflict-of-Interest Policy, the authors have indicated no other relevant relationships that could be perceived as a real or apparent conflict of interest. Disclosure of a relationship is not intended to suggest or to condone bias but is made to provide participants with information that might be of potential importance to their evaluation of the activity.
CME Credit: SNMMI is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to sponsor continuing education for physicians. SNMMI designates each JNM continuing education article for a maximum of 2.0 AMA PRA Category 1 Credits. Physicians should claim only credit commensurate with the extent of their participation in the activity. For CE credit, SAM, and other credit types, participants can access this activity through the SNMMI website (http://www.snmmilearningcenter.org) through April 2026.
- © 2023 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication December 21, 2022.
- Revision received February 2, 2023.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}